Non-Occlusive Mesenteric Ischemia (NOMI): Diagnosis, ICU Management, and Clinical Pitfalls
Introduction
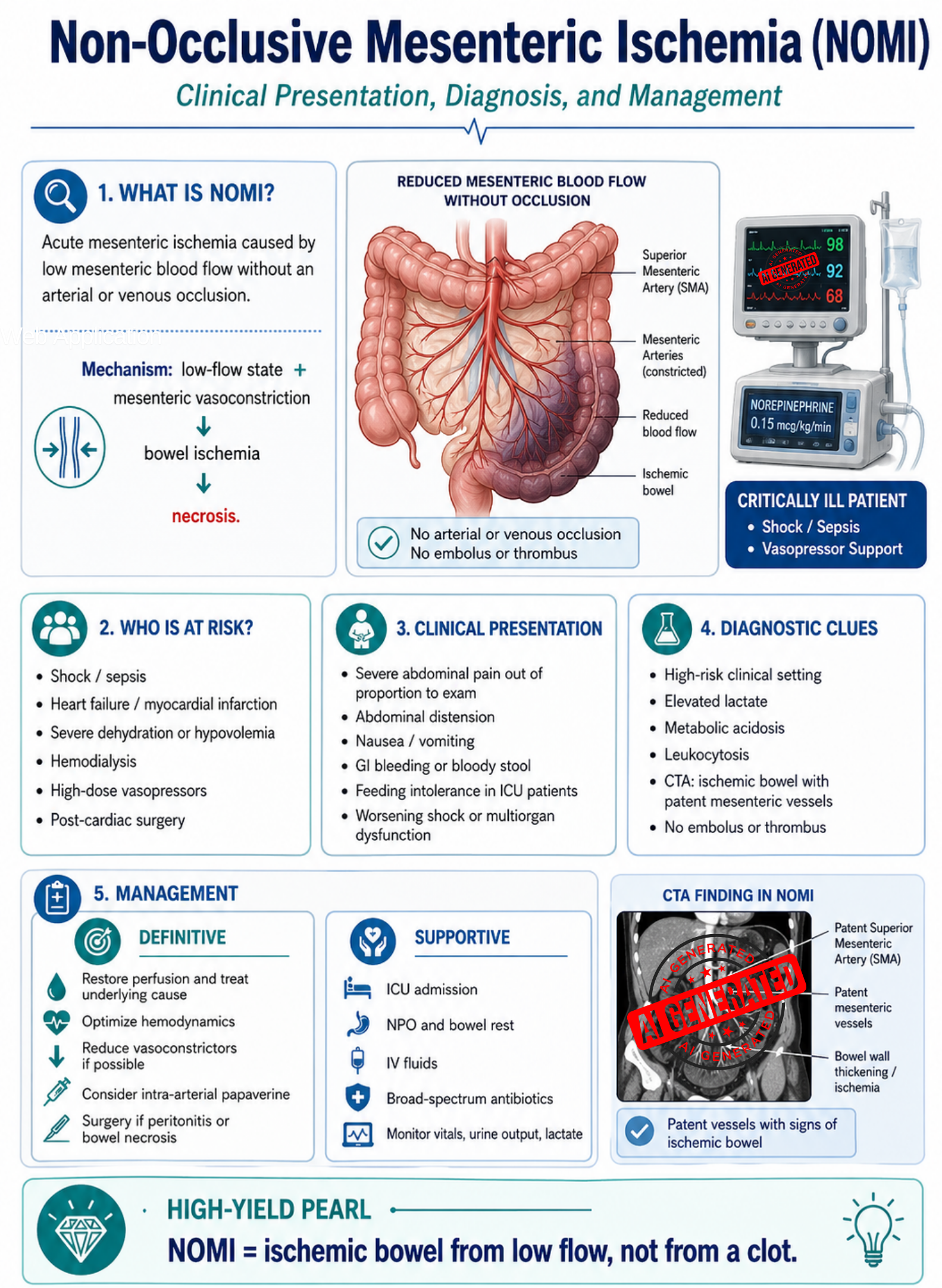
Non-occlusive mesenteric ischemia, or NOMI, is a life-threatening form of acute mesenteric ischemia in which the bowel becomes ischemic without an obstructing thrombus or embolus in the mesenteric vessels. The core problem is low intestinal blood flow, usually from shock, severe cardiac dysfunction, hypovolemia, sepsis, or excessive vasoconstriction from vasopressors. The World Society of Emergency Surgery describes NOMI as a condition commonly caused by superior mesenteric artery vasoconstriction with low splanchnic blood flow, often in critically ill patients. (Springer Link)
Clinically, NOMI should be treated as an ICU-level emergency, not an OPD problem. The dangerous feature is that early symptoms may be subtle, especially in sedated or ventilated ICU patients, while bowel necrosis can progress rapidly.
Pathophysiology
The intestine normally receives a large blood supply, especially after meals. In shock states, the body prioritizes blood flow to the heart and brain. To maintain central circulation, the body constricts blood vessels in the skin, kidneys, and gut.
In NOMI, this compensatory vasoconstriction becomes harmful:
Low-flow state → mesenteric vasoconstriction → mucosal hypoxia → bowel wall ischemia → necrosis → perforation, sepsis, multiorgan failure
Unlike embolic or thrombotic acute mesenteric ischemia, the main mesenteric arteries may remain patent on imaging. The bowel is ischemic because the blood flow is too low or too constricted, not because a large vessel is blocked.
Common precipitating factors include:
- Septic shock
- Cardiogenic shock
- Severe heart failure
- Myocardial infarction
- Post-cardiac surgery state
- Hemodialysis
- Severe dehydration or hypovolemia
- High-dose vasopressor therapy
- Vasoconstrictive drugs such as norepinephrine, epinephrine, vasopressin, or digoxin
WSES specifically notes cardiac failure, sepsis, hypovolemia, and vasoconstrictive agents as important precipitants of NOMI. (Springer Link)
Clinical Presentation
Classic presentation
The classic presentation of acute mesenteric ischemia is:
Severe abdominal pain out of proportion to the physical examination
This occurs because ischemia begins in the intestinal mucosa before the serosa and peritoneum become inflamed. Early in the disease, the patient may have severe pain but only mild abdominal tenderness. WSES recommends that severe abdominal pain out of proportion to examination findings should be assumed to be acute mesenteric ischemia until proven otherwise. (Springer Link)
Symptoms
Patients may present with:
- Severe diffuse abdominal pain
- Abdominal distension
- Nausea and vomiting
- Diarrhea
- Bloody stool or maroon stool
- Feeding intolerance in ICU patients
- Unexplained metabolic acidosis
- Worsening shock
- New or worsening multiorgan dysfunction
In sedated, ventilated, or critically ill patients, abdominal pain may be absent or impossible to assess. In these cases, warning signs may be only abdominal distension, gastrointestinal bleeding, worsening organ failure, increasing vasopressor requirement, or intolerance of enteral feeding. WSES emphasizes that routine clinical examination and laboratory tests have limited value for early NOMI diagnosis. (Springer Link)
Physical examination findings
Early findings may be minimal:
- Soft abdomen
- Mild tenderness
- Pain much worse than expected from examination
Late findings suggest bowel infarction:
- Guarding
- Rebound tenderness
- Rigidity
- Absent bowel sounds
- Fever
- Shock
- Peritonitis
Exam pearl: ✅ Early NOMI = severe ischemia with minimal abdominal signs ❌ Late NOMI = peritonitis, necrosis, perforation, septic shock
Peritoneal signs strongly suggest transmural bowel necrosis and require urgent surgical evaluation. (Springer Link)
Diagnostic Criteria
There is no single laboratory test that confirms NOMI. Diagnosis is based on a combination of clinical suspicion, risk factors, laboratory deterioration, and imaging evidence of bowel ischemia without occlusive arterial or venous blockage.
Practical diagnostic criteria for NOMI
NOMI should be strongly suspected when all or most of the following are present:
- High-risk clinical setting
- Shock, sepsis, heart failure, post-cardiac surgery, dialysis, severe dehydration, or high-dose vasopressor use.
- Compatible clinical deterioration
- Abdominal pain, abdominal distension, GI bleeding, feeding intolerance, worsening shock, or new multiorgan dysfunction.
- Laboratory evidence of hypoperfusion or inflammation
- Elevated lactate
- Metabolic acidosis
- Leukocytosis
- Elevated D-dimer may support suspicion but is not diagnostic.
- CTA findings compatible with ischemia
- Bowel wall hypoenhancement
- Bowel dilatation
- Bowel wall thickening or thinning
- Pneumatosis intestinalis
- Portal venous gas
- Free intraperitoneal fluid
- Patent mesenteric vessels without arterial embolus, arterial thrombosis, or mesenteric venous thrombosis
- No mechanical occlusion
- No SMA embolus
- No SMA thrombosis
- No mesenteric venous thrombosis explaining the ischemia
WSES states that CTA in NOMI may show bowel ischemia and free fluid despite patent mesenteric vessels, and diagnostic angiography can help distinguish occlusive from non-occlusive mesenteric ischemia. (Springer Link)
Laboratory Evaluation
Laboratory tests are useful for severity assessment, but they cannot reliably rule in or rule out NOMI.
Important tests include:
- CBC: leukocytosis may be present
- Serum lactate: elevated in hypoperfusion or necrosis
- ABG or VBG: metabolic acidosis
- Electrolytes, BUN, creatinine: dehydration, renal injury, baseline before contrast
- LFTs
- Coagulation profile
- Blood culture if sepsis is suspected
- Type and screen / crossmatch if surgery is possible
WSES states that no laboratory parameter is sufficiently accurate to conclusively identify ischemic or necrotic bowel, although leukocytosis, elevated lactate, and D-dimer may support suspicion. Lactate elevation should not be used alone to decide whether bowel necrosis is present. (Springer Link)
Important clinical pearl: ❌ Normal lactate does not safely exclude early NOMI. ✅ Rising lactate plus abdominal symptoms or unexplained shock should trigger urgent CTA.
Imaging Diagnosis
First-line investigation: CT angiography
CTA abdomen and pelvis with arterial and venous phases is the key diagnostic test when NOMI or any acute mesenteric ischemia is suspected.
WSES gives a strong recommendation that CTA should be performed without delay in any patient with suspected acute mesenteric ischemia. The guideline also states that delay in CTA is strongly associated with mortality and that multidetector CTA has replaced formal angiography as the diagnostic study of choice. (Springer Link)
CTA should evaluate:
- Arterial occlusion
- Venous thrombosis
- Bowel wall enhancement
- Bowel wall thickness
- Pneumatosis intestinalis
- Portal venous gas
- Mesenteric edema
- Free fluid
- Perforation
Role of catheter angiography
Catheter angiography is less commonly the first diagnostic test now, but it remains useful when:
- CTA is equivocal
- NOMI is strongly suspected
- Catheter-directed vasodilator therapy is being considered
- Interventional radiology is available
The ACR radiologic management update states that for NOMI, transarterial infusion of vasodilators such as papaverine or prostaglandin E1 is the recommended initial interventional treatment. (ScienceDirect)
Management
Management setting
NOMI should be managed as an inpatient ICU emergency.
✅ Correct setting: IPD / ICU ❌ Incorrect setting: OPD management
The main goals are:
- Restore mesenteric perfusion
- Correct the underlying shock state
- Prevent progression to bowel necrosis
- Resect necrotic bowel if present
- Prevent sepsis and multiorgan failure
Initial Stabilization
1. Resuscitation
Start immediately when NOMI is suspected:
- NPO
- Two large-bore IV lines or central venous access
- Isotonic crystalloid resuscitation, such as 0.9% normal saline IV bolus, guided by blood pressure, urine output, lactate, and cardiac function
- Correct electrolyte abnormalities
- Insert Foley catheter to monitor urine output
- Serial abdominal examination
- Monitor vital signs continuously
- Monitor lactate trend and acid-base status
WSES recommends immediate fluid resuscitation to improve visceral perfusion, correction of electrolyte abnormalities, nasogastric decompression, and hemodynamic monitoring. (Springer Link)
2. Bowel rest and decompression
- Keep patient NPO
- Insert nasogastric tube if vomiting, ileus, or significant distension
- Stop enteral feeding in critically ill patients if NOMI is suspected
Supportive measures such as nasogastric suction, fluid resuscitation, and bowel rest are part of acute mesenteric ischemia care. (Springer Link)
3. Broad-spectrum antibiotics
Give early antibiotics because ischemic bowel loses its mucosal barrier, allowing bacterial translocation.
Example adult regimen, assuming normal renal function:
- Piperacillin-tazobactam 4.5 g IV every 6 hours
Alternative:
- Ceftriaxone 2 g IV once daily + metronidazole 500 mg IV every 8 hours
WSES recommends immediate broad-spectrum antibiotics in acute mesenteric ischemia and notes that antibiotic therapy should generally continue for at least 4 days in stable immunocompetent patients, with longer duration if ongoing infection is present. (Springer Link)
Definitive Treatment
1. Correct the underlying cause
This is the core treatment of NOMI.
Definitive management includes:
- Treat sepsis aggressively
- Restore intravascular volume
- Optimize cardiac output
- Correct hypoxia and anemia
- Reduce or stop vasoconstrictive drugs if possible
- Avoid excessive vasopressin when alternatives are available
- Use inotropes when cardiac output is poor, guided by ICU assessment
WSES states that the central principle of NOMI management is treatment of the precipitating cause, including fluid resuscitation, optimization of cardiac output, and elimination of vasopressors when possible. (Springer Link)
2. Catheter-directed vasodilator therapy
If there is no peritonitis or perforation and interventional radiology is available, consider:
- Intra-arterial papaverine infusion into the SMA
- Or prostaglandin E1 where used by local protocol
This directly targets mesenteric vasospasm.
WSES notes that catheter-directed vasodilatory and antispasmodic therapy, most commonly papaverine, may be used in NOMI. However, it also notes that real-world use is variable and evidence is based mainly on small studies and selected cohorts. (Springer Link)
3. Surgery
Urgent surgery is required if there is evidence of:
- Peritonitis
- Perforation
- Frank bowel necrosis
- Clinical deterioration despite resuscitation
- Worsening lactic acidosis
- Sepsis from suspected infarcted bowel
Surgery includes:
- Exploratory laparotomy or selected diagnostic laparoscopy
- Assessment of bowel viability
- Resection of non-viable bowel
- Damage-control surgery if unstable
- Second-look laparotomy after 24–48 hours when bowel viability is uncertain
WSES states that infarcted bowel should be promptly resected and that exploratory laparotomy is required when peritoneal signs are present. (Springer Link)
Monitoring and Complications
Monitoring
Patients need ICU-level monitoring:
- Vital signs
- Urine output target generally ≥0.5 mL/kg/hour
- Serial abdominal examinations
- Lactate every 2–4 hours initially
- ABG/VBG for acidosis
- CBC, electrolytes, renal function
- Vasopressor requirement
- Signs of GI bleeding
- Repeat CTA or second-look surgery if deterioration occurs
Complications
Major complications include:
- Bowel necrosis
- Perforation
- Peritonitis
- Sepsis
- Septic shock
- Multiorgan failure
- Short bowel syndrome after extensive resection
- Death
Mortality remains high, especially once peritonitis or bowel necrosis develops. WSES reports very high mortality in patients with peritoneal signs, reflecting advanced ischemia and critical illness. (Springer Link)
Exam-Friendly Summary
NOMI = bowel ischemia from low flow, not from a clot.
Suspect NOMI in:
✅ ICU patient ✅ Shock or heart failure ✅ High-dose vasopressors ✅ Abdominal distension or GI bleeding ✅ Rising lactate or metabolic acidosis ✅ CTA shows ischemic bowel but patent mesenteric vessels
Do not wait for:
❌ Classic abdominal pain in sedated ICU patients ❌ A diagnostic lactate threshold ❌ Plain abdominal X-ray confirmation ❌ Peritonitis before ordering CTA
Correct management:
✅ ICU admission ✅ Fluid resuscitation ✅ Optimize cardiac output ✅ Reduce vasopressors if possible ✅ Broad-spectrum antibiotics ✅ CTA without delay ✅ Consider SMA catheter papaverine ✅ Surgery if peritonitis, perforation, necrosis, or deterioration
Conclusion
Non-occlusive mesenteric ischemia is one of the most easily missed but most dangerous abdominal emergencies in critically ill patients. The diagnosis depends on clinical suspicion, especially in patients with shock, vasopressor use, cardiac failure, sepsis, or dialysis. Laboratory tests can support suspicion but cannot exclude the disease. CTA should be performed urgently, and management must focus on restoring intestinal perfusion, treating the underlying low-flow state, giving broad-spectrum antibiotics, and proceeding to surgery when bowel necrosis or peritonitis is suspected.
High-yield memory line: NOMI = No Occlusion, Mesenteric Ischemia from low-flow vasoconstriction.